MUST READ – Why small things matter : the scientific indisputable proof and why it matters
10 Key
Practical Takeaway Points: Applying Chaos Theory to Clinical Practice
1. Accept
Uncertainty as Fundamental — Stop
viewing unpredictability as a failure of medical knowledge. Uncertainty is
inherent in complex adaptive systems, not a deficiency to eliminate. This
reframe allows you to practice with authenticity.
2. Small
Compassionate Acts Matter Disproportionately — The butterfly effect demonstrates that tiny
interventions—a validating comment, a moment of empathic listening, a pause to
acknowledge fear—can ripple through patient experience in ways you cannot
predict or trace. Never underestimate the power of presence.
3. Acknowledge
Rather Than Dismiss — Be
honest about what you don’t know. Patients consistently report that authentic
acknowledgment of uncertainty (balanced with hope and structure) builds trust
more effectively than false reassurance. Honesty is therapeutic.
4. Look for
Strange Attractors in Team Dynamics — Recognize that teams develop stable patterns: “the
way we do things here.” To change dysfunctional culture, identify the
underlying rules, assumptions, and feedback loops that reinforce current
behaviors, then deliberately alter them.
5. Establish
Simple Rules, Not Complex Protocols — Replace elaborate top-down directives with a few clear,
locally-applied principles: “Speak up about safety concerns,”
“Seek to understand before judging,” “Share transparently.”
Sophisticated collaborative behavior emerges naturally from simple rules.
6. Create
Short Feedback Loops —
Healthcare systems suffer from long delays between actions and consequences.
Use regular team debriefs, incident reviews, and peer reflection to accelerate
feedback. This allows the system to self-correct before damage accumulates.
7. Operate
at the Edge of Chaos —
Excessive rigidity creates brittleness; complete chaos destroys function. The
optimal zone for creativity and adaptation lies between these extremes. Foster
conditions for safe experimentation while maintaining enough structure for
coherence.
8. Validate
Emotions and Uncertainty in Consultations — When patients experience fear and sense ambiguity,
acknowledge it rather than deny it. Name the chaos while anchoring them in the
pattern (typical course, structure of ongoing support). This dual approach
reduces anxiety more than reassurance alone.
9. Manage
Contexts, Not Outcomes — Stop
trying to engineer specific trajectories through detailed control. Instead,
establish clear strategic aims and core values, grant frontline teams autonomy
in pursuit of those aims, and invest in communication infrastructure.
Management becomes gardening, not engineering.
10. Be
Present for the Butterfly’s Flap — You cannot guarantee which small act will catalyze
transformation, but you can commit to showing up consistently, compassionately,
and authentically. The patterns—the strange attractors—will organize themselves
around your presence and intention.
Chaos, Patterns, and Compassion: What
Chaos Theory Teaches Us About Clinical Practice
When I first encountered chaos theory
during my musings in physics, I dismissed it as an abstract mathematical
curiosity—butterfly wings causing hurricanes seemed far removed from the world
of clinical oncology. The more I read about the chaos theory , its implications
across all fields of science , not just physics and the more I’ve reflected on
my interactions with patients, colleagues, and the healthcare system itself,
the more I’ve realized that chaos theory offers profound insights into the
daily reality of medical practice.
We operate in medicine as if we live in
a deterministic, predictable universe. We follow protocols, calculate risk scores, and design
treatment algorithms with the implicit assumption that knowing the initial
conditions—stage, grade, performance status, biomarkers—should allow us to
predict outcomes with reasonable accuracy. But chaos theory tells us something
unsettling: even in purely deterministic systems governed by fixed rules,
long-term prediction can be impossible. Small differences in initial conditions
diverge exponentially over time, rendering detailed forecasts futile beyond a
certain horizon. This phenomenon, famously termed the “butterfly
effect,” suggests that the flap of a butterfly’s wings in Brazil might
theoretically set off a tornado in Texas.[1][2][3][4]
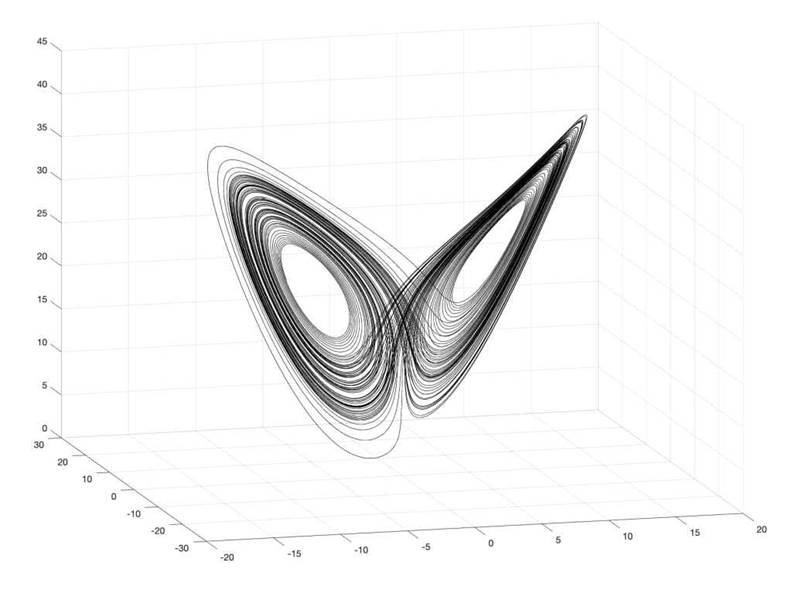
Edward Lorenz’ Chaotic Butterfly |
Galileo Unbound
Yet here lies the paradox that has
captivated me: chaos is not randomness.
Within the apparent unpredictability, patterns emerge—stable structures called
“strange attractors” that constrain the system’s behavior even when
we cannot predict its exact trajectory. The system wanders unpredictably,
yet never wanders anywhere. It
traces out a recognizable shape in its state space, returning again and again
to familiar regions without ever repeating exactly.[5][4][6][7][8]
The Consultation as a Complex Adaptive
System
Consider the clinical consultation. On
the surface, it appears straightforward: a patient presents with symptoms, we
gather history and examination findings, order investigations, synthesize the
data, and formulate a management plan. Linear cause and effect. Simple
input-output mechanics.
But every experienced clinician knows
this is fantasy. The consultation is a
complex adaptive system—a dynamic interaction where patient and doctor
mutually influence each other in nonlinear ways. The doctor’s tone affects
the patient’s willingness to disclose; the patient’s anxiety shapes the
doctor’s communication style; unspoken fears create feedback loops that amplify
or dampen information exchange. Small changes within or external to this system
can lead to major shifts in the overall dynamic, while large interventions
sometimes make surprisingly little difference.[9][1][10]
Research into complexity theory in
general practice has shown that consultations exist in a “zone of
complexity”—far from the certainty and agreement that would allow
mechanistic problem-solving, yet not so chaotic that no progress can be
made. This is the space where most of oncology practice actually happens. We
deal with ambiguous symptoms, conflicting evidence, patient values that don’t
align neatly with guideline recommendations, and prognoses shrouded in
statistical uncertainty.[1][11][9]
Understanding the consultation as a
complex adaptive system provides a theoretical basis for what we intuitively
know: outcome is essentially
unpredictable in its details. We cannot script a consultation and expect it
to unfold as planned. The patient may reveal something unexpected in the final
minute that reframes everything. A seemingly minor comment may unlock a
therapeutic relationship, or inadvertently damage it. Non-linearity means
that a carefully prepared explanation might fall flat, while an offhand
reassurance might prove transformative.[9][1][2]
The Butterfly Effect in Clinical
Interactions
The butterfly effect carries profound
implications for how we interact with patients, colleagues, and management. In
one striking account from psychiatric practice, a clinician described initially
embracing the butterfly effect as a source of hope—the belief that even the
smallest intervention could create a tsunami of positive change on the other
side. After deeper study, however, she discovered her interpretation had been
backwards. The butterfly effect is not
about leverage or predictable amplification. It is about sensitivity to
initial conditions: a butterfly’s flap can
trigger a cascade, but only if it occurs at precisely the right place and time
where environmental conditions allow such an outcome.[2][12]
This realization transforms how we
approach clinical work. It means we cannot reliably engineer large outcomes
through small, calculated interventions. We lack the precision to know which
initial conditions will amplify and which will dissipate. Yet paradoxically,
this same insight underscores the critical
importance of every small action.
Without the butterfly’s flap—without our compassionate word, our moment of
listening, our empathic acknowledgment—there is no possibility of change at
all. The cascade may not materialize, but its absence is guaranteed
without the initial perturbation.[13][2]
Studies in oncology communication bear
this out. When oncologists respond to patients’ negative emotions with empathy,
patients perceive the communication more favorably, despite the emotions
themselves being difficult. Clinicians’ communication focused on managing
uncertainty and responding to emotions predicts better patient health, improved
coping, and reduced psychological distress, even after controlling for other
factors. These are not grand gestures. They are small moments—a pause, a
validating statement, an expression of support—yet they ripple through the
patient’s experience in ways we cannot fully trace or predict.[14][15][16][17][18][2]
Strange Attractors in Healthcare
Systems
If the butterfly effect describes
sensitivity in the moment, strange attractors describe the patterns that emerge over time in
complex systems. In biological systems, attractors represent structured
patterns of behavior despite persistent noise and perturbation. Body
temperature returns to normal after exertion; hormone levels regulate despite
irregular supply and demand. In disease states, the system may shift to a
different attractor—chronic illness represents a stable state that resists
perturbation back to health, just as health itself resists perturbation toward
disease.[5][19][6][7]
This attractor metaphor offers a
powerful lens for understanding organizational dynamics in healthcare. Teams,
departments, and institutions develop stable patterns of interaction—”the
way we do things here”—that persist even when individuals come and go.
These attractors can be functional or dysfunctional. A culture of blame
creates a powerful attractor that pulls new team members into defensive
behaviors. Conversely, a culture of psychological safety creates an
attractor for open communication and learning.[20][21][10]
Transformational
change involves creating new contexts that break the hold of dominant
attractors in favor of new ones. This is not about issuing new policies or restructuring
the organizational chart. It is about identifying the simple rules,
underlying assumptions, and feedback loops that reinforce existing patterns,
and deliberately altering them. It is about managing contexts rather than
trying to control outcomes.[22][21][10][20]
For example, if the dominant
attractor in a clinical team is “always defer to the consultant,”
then attempts to promote shared decision-making will fail unless the underlying
rules change. The consultant must actively solicit input, visibly value
dissenting opinions, and create safety for junior colleagues to speak up. These
behavioral shifts alter the attractor basin, allowing new patterns of
collaboration to emerge. Notably, the
outcome remains unpredictable—we cannot determine exactly how the team
will reorganize itself—but we can create conditions that favor healthier
dynamics.[21][10][23][24][20]
Navigating
the Edge of Chaos
Chaos theory describes a state called the
“edge of chaos”—a zone of optimal creativity and adaptability where a
system is neither rigidly ordered nor completely chaotic. At one extreme,
excessive order creates brittleness; the system cannot respond to novelty or
disruption. At the other extreme, chaos overwhelms; nothing can be accomplished
because there is no structure to build upon. The edge of chaos is the fertile ground
between these poles, where sufficient structure exists to enable action, yet
sufficient flexibility exists to allow innovation.[9][1][25][26]
Complex consultations sometimes enter
this zone. When a
consultation moves from safe, familiar territory—discussing straightforward
treatment options—into less charted waters—acknowledging existential fears,
exploring end-of-life values, surfacing conflicts between patient and
family—the interaction becomes unstable in a productive sense. There is
risk: the doctor-patient relationship might be strengthened through deeper
understanding, or it might fracture if either party feels threatened. This
instability, this venture into the unknown, is where meaningful transformation
can occur.[20][27][9]
The same principle applies to
organizational change.
Healthcare systems facing unprecedented challenges—budget constraints,
workforce shortages, evolving patient expectations—must operate at the edge of
chaos to survive. Too much rigidity and they collapse under the weight of
inflexible structures unsuited to new realities. Too much chaos and they
fragment into dysfunction. The optimal zone allows for experimentation,
learning, and adaptation while maintaining enough coherence to deliver care.[1][25][26][28]
Leaders in this environment cannot rely
on command-and-control approaches. They must foster
conditions for self-organization: establishing simple rules, ensuring open
communication, providing autonomy within clear boundaries, and creating
psychological safety for risk-taking. Crucially, they must tolerate the
discomfort of not knowing exactly how things will unfold—what complexity
theorists call “the good-enough holding of anxiety”.[21][23][29][9][1][20]
Practical Implications for Clinical
Interactions
What does all this mean for daily
practice? How can understanding chaos theory improve our interactions with
patients, colleagues, and management?
With Patients: Embrace Uncertainty
While Offering Structure
Chaos theory validates what patients
intuitively sense: uncertainty is inherent, not a failure of
medical knowledge. Rather than projecting false certainty—”the
treatment will work” when we mean “there’s a 60% response
rate”—we can acknowledge the unpredictability while emphasizing the
patterns. “I cannot tell you exactly what will happen for you, but I can
tell you what the typical course looks like, and I will be with you whatever
unfolds.”[9][1][11][14]
This honest acknowledgment of
uncertainty, paradoxically, builds trust and reduces anxiety more effectively than false reassurance. Patients
navigating cancer treatment crave authenticity balanced with hope. They need us
to name the chaos—the unknowns, the “what ifs,” the divergent
possibilities—while simultaneously anchoring them in the patterns, the
attractor around which their journey will likely revolve.[5][14][15][30][17]
Small communicative acts matter
profoundly.
Validating emotions, expressing empathy, checking understanding, inviting
questions—these micro-interventions shape the system’s trajectory in ways
disproportionate to their size. We may not predict which moment will prove
pivotal, but we create the conditions for positive change through consistent
compassionate engagement.[2][14][15][16]
With Colleagues: Foster Simple Rules
and Feedback Loops
Complex adaptive systems function well
when agents follow a few simple, locally applied rules rather than elaborate
top-down directives. In healthcare teams, simple rules might include:
“Speak up if you see a safety concern,” “Seek to understand
before judging,” “Share information transparently,”
“Acknowledge when you don’t know”. These rules, consistently applied,
allow sophisticated collaborative behavior to emerge without micromanagement.[23][29][24]
Crucially, feedback must be visible and timely. Complexity in healthcare
arises partly from long delays between actions and consequences—a
communication breakdown today may only surface as a patient complaint months
later. Shortening feedback loops through regular team debriefs, incident
reviews, and peer reflection helps the system self-correct.[1][20][31][23]
Beware of the attractor of professional
tribalism.
Medicine, nursing, pharmacy, and administration often operate in silos, each
with its own culture and priorities. Breaking these attractors requires
deliberate efforts to create shared goals, interdisciplinary forums, and mutual
respect. Leaders must model the new pattern: visibly valuing diverse input,
deferring to expertise regardless of hierarchy, and framing challenges as
collective problems rather than jurisdictional disputes.[32][20][21][10][33]
With Management: Balance Order and
Flexibility
Healthcare organizations face the
temptation to impose rigid protocols in response to complexity—”if only we had the right
algorithm, the right flowchart, the right checklist, then outcomes would be
predictable”. But chaos theory reminds us that detailed control is impossible in complex adaptive systems.
Over-specification stifles adaptation.[9][1][20][25][26]
The alternative is not abdication of
responsibility, but rather management
of contexts and enabling conditions.
Define clear strategic aims and core values (the attractor you want the
organization to orbit), then grant frontline teams autonomy in how they pursue
those aims. Invest in communication infrastructure so that
learning propagates rapidly across the system. Encourage safe-to-fail
experiments where innovations can be tested without catastrophic risk.[20][21][34][23][25][26][29]
This approach accepts that change will
be emergent and somewhat unpredictable, but channels it toward desirable
outcomes. It replaces the illusion of control with the reality of influence. Managers
become gardeners, cultivating conditions for growth, rather than engineers,
constructing predetermined structures.[1][21][25][20]
Conclusion: Living with Chaos, Guided
by Patterns
Chaos theory does not counsel nihilism. It does not say “nothing
matters” or “anything can happen.” Rather, it articulates a more
nuanced truth: the detailed future is
unknowable, yet deeply patterned. We navigate by recognizing the
attractors—the recurring themes, the stable dynamics, the boundaries of
possibility—while releasing the illusion that we can script the journey step
by step.[5][4][6][7][8]
In clinical practice, this means
accepting uncertainty as a fundamental feature, not a problem to be solved. It means valuing small
compassionate acts, knowing they shape the system even when we cannot
trace their effects. It means fostering conditions for emergence—simple rules,
open communication, psychological safety—rather than imposing rigid structures.
And it means embracing the edge of chaos, where discomfort and creativity
coexist, as the space where meaningful change becomes possible.[9][1][20][2][11][23][25][26][14][15]
The next time a consultation takes
an unexpected turn, or a team dynamic shifts in surprising ways, or an
organizational initiative unfolds differently than planned, perhaps we can
pause and recognize: we are witnessing chaos. Not randomness, not failure,
but a complex adaptive system doing what such systems do—evolving unpredictably
within deep patterns, sensitive to small perturbations, constrained by hidden
attractors. Our role is not to control the chaos, but to participate
thoughtfully within it, cultivating the conditions where healing,
collaboration, and positive transformation become more likely.
In the end, chaos theory offers
medicine a gift: permission to be humble
about prediction, yet confident in presence. We may not know where
the butterfly’s flap will lead, but we can commit to being present for the flap
itself—for the compassionate word, the empathic pause, the vulnerable question,
the courageous experiment. These small acts are not guaranteed to
produce proportional results, but they are the necessary precursors to any
change at all. And the patterns will take care of themselves.
1.
https://pmc.ncbi.nlm.nih.gov/articles/PMC1121189/
2.
https://www.statnews.com/2023/08/30/youth-mental-health-crisis-chaos-theory-child-psychology/
3.
https://en.wikipedia.org/wiki/Butterfly_effect
4.
https://en.wikipedia.org/wiki/Chaos_theory
5.
https://library-of-atlantis.com/2023/08/26/strange-attractors/
6.
https://brucewlee.com/blog/posts/strange-attractors.html
7.
https://extendednows.com/attractors-the-platform-for-creating-new-futures-in-chaotic-systems/
8.
https://sharkfreewaters.com/2012/09/05/strange-attractor-patterns-chaos-theory-and-change/
9.
https://pmc.ncbi.nlm.nih.gov/articles/PMC1266243/
10.
https://journals.library.ualberta.ca/complicity/index.php/complicity/article/download/8727/7047
11.
https://pmc.ncbi.nlm.nih.gov/articles/PMC6925325/
12.
https://unwantedlife.me/the-interesting-applications-of-chaos-theory-on-our-wellbeing
13.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8187700/
14.
https://www.cancer.gov/about-cancer/coping/adjusting-to-cancer/communication-hp-pdq
15.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8968177/
16.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8557158/
17.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7229568/
18.
https://www.sciencedirect.com/science/article/abs/pii/S0738399122001434
19.
https://pmc.ncbi.nlm.nih.gov/articles/PMC8085613/
20. https://realkm.com/2019/03/18/exploring-the-science-of-complexity-series-part-16-concept-7-strange-attractors-and-the-edge-of-chaos/
21.
https://www.lifeleadership.uk/attractors/
22. https://www.hsdglobalservices.org/resources/hsd-in-the-world-a-strange-attractor-pattern.html
23. https://www.linkedin.com/pulse/three-properties-complex-adaptive-systems-influence-advisor–2mnhf
24. https://onlinelibrary.wiley.com/doi/full/10.1111/jep.12878
25. https://measuremen.io/blog/the-holy-grail-of-innovation-the-edge-of-chaos/
26. https://pmc.ncbi.nlm.nih.gov/articles/PMC1279501/
27.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10423463/
28. https://www.sciencedirect.com/science/article/pii/S2514664524000146
29. https://www.ncbi.nlm.nih.gov/books/NBK222267/
30. https://www.cancercarepune.com/strategies-for-coping-with-uncertainty-in-cancer-treatment/
31.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10970665/
32. https://internationaljournalofcaringsciences.org/docs/72_karaman_special_12_2-22.pdf
33. https://pmc.ncbi.nlm.nih.gov/articles/PMC9598193/
34. https://nobl.io/changemaker/gareth-morgan-organizational-metaphors/
35. https://cancercontrol.cancer.gov/sites/default/files/2020-06/pcc_monograph.pdf
36. https://self-compassion.org/wp-content/uploads/publications/nurseselfcare.pdf
37.
https://www.news-medical.net/health/How-to-Foster-a-People-Centered-Environment-in-Cancer-Treatment.aspx
38. https://cancersupportuk.org/conversations-about-cancer-a-guide-to-compassionate-communication/
39. https://chti.upenn.edu/tiny-flaps-big-waves-drawing-parallels-between-butterfly-effect-and-health-care-innovation
40. https://acsjournals.onlinelibrary.wiley.com/doi/full/10.1002/cncr.32823
42. https://www.ajan.com.au/index.php/AJAN/article/download/2406/865/12370
43. https://www.thieme-connect.com/products/ejournals/pdf/10.1055/s-0040-1703623.pdf
44. https://www.sciencedirect.com/science/article/pii/S1658361225000587
45. https://www.jungiananalysts.org.uk/wp-content/uploads/2016/10/Van-Eenwyk-J.-Archetypes-The-Strange-Attractors-of-the-Psyche.pdf
46. https://www.scirp.org/journal/paperinformation?paperid=132410
47. https://www.bmj.com/content/303/6817/1565
48. https://www.sciencedirect.com/science/article/abs/pii/S0001879107000553
49. https://pmc.ncbi.nlm.nih.gov/articles/PMC5378487/
50. https://sk.sagepub.com/ency/edvol/medical/chpt/chaos-theory
51.
https://www.sciencedirect.com/science/article/pii/S2589871X25000166
52. https://medcraveonline.com/BBIJ/chaotic-attractors-in-cancer-and-epidemic-models-insights-from-predator-prey-interactions.html
53. https://www.bmj.com/rapid-response/2011/10/28/chaos-and-complexity-based-health-system
54. https://thecynefin.co/superbugs-strange-attractors-and-resilience/
55.
https://www.reddit.com/r/FamilyMedicine/comments/14ed6fh/practicechanging_journal_articles/
56. https://pubmed.ncbi.nlm.nih.gov/38382001/
57.
https://www.sciencedirect.com/science/article/abs/pii/S1462388911001840
58. https://news.bms.com/news/details/2020/CheckMate–649-a-Phase-3-Trial-Evaluating-Opdivo-nivolumab-Plus-Chemotherapy-vs.-Chemotherapy-Meets-Primary-Endpoints-Demonstrating-Superior-Overall-Survival-and-Progression-Free-Survival-in-First-Line-Treatment-of-Gastric-and-Esophageal-Cancers/default.aspx
59. https://pmc.ncbi.nlm.nih.gov/articles/PMC3170054/
60. https://pmc.ncbi.nlm.nih.gov/articles/PMC11185916/
61.
https://www.sciencedirect.com/science/article/abs/pii/S0736467925003828
62. https://ascopubs.org/doi/10.1200/JCO.2017.35.15_suppl.TPS4132
63. https://oncologyjc.blogspot.com
64. https://gist.cl/wp-content/uploads/2021/06/1-s2.0-S0140673621007972-main.pdf
65. https://pmc.ncbi.nlm.nih.gov/articles/PMC2790637/
66. https://trials.cancervic.org.au/details/vctl_nct02872116
67. https://pdfs.semanticscholar.org/af4e/944089684b36562c16cd7a9c747011268f54.pdf
68. https://perfilesycapacidades.javeriana.edu.co/en/publications/a-plain-language-summary-of-the-checkmate-649-study-nivolumab-in-/
69. https://praxisoncology.com/index.php/TPO/about
70. https://perfilesycapacidades.javeriana.edu.co/es/publications/a-plain-language-summary-of-the-checkmate-649-study-nivolumab-in-
71.
https://www.practiceupdate.com/Explore/Index
72.
https://www.personalizedmedonc.com/special-issues/clinical-trials-to-clinical-practice-gi-cancer-edition/234391:clinical-trials-to-clinical-practice-gi-cancer-edition
73.
https://jhm.qa00.mdedge.com/hematology-oncology/clinical-insights
74. https://pubmed.ncbi.nlm.nih.gov/35687005/
75.
https://www.magonlinelibrary.com/doi/abs/10.12968/jpar.2023.15.4.CPD1
76. https://dergipark.org.tr/tr/download/article-file/109714
77.
https://www.tandfonline.com/doi/full/10.1080/13698575.2025.2492147
78. https://pmc.ncbi.nlm.nih.gov/articles/PMC12176066/
79. https://pmc.ncbi.nlm.nih.gov/articles/PMC2446457/
80. https://gh.bmj.com/content/4/Suppl_1/e000899
81.
https://www.linkedin.com/posts/helenbevanhealthcare_organisational-change-is-happening-at-a-scale-activity-7353120791166681090-B5is
82. https://study.com/academy/lesson/chaos-theory-in-psychology.html
83. https://www.sciencedirect.com/science/article/pii/S0169207017301346
84. http://samples.jbpub.com/9781284050684/9781284034288_CH01.pdf
85. https://iahip.org/page-1075736
86. https://asmepublications.onlinelibrary.wiley.com/doi/full/10.1111/tct.13165
87. https://pmc.ncbi.nlm.nih.gov/articles/PMC3445676/
88. https://www.bmj.com/content/374/bmj.n2061
89. https://www.physio-pedia.com/International_Framework_for_Examination_of_the_Cervical_Region
90. https://www.england.nhs.uk/improvement-hub/wp-content/uploads/sites/44/2017/11/Creating-the-Culture-for-Innovation-Practical-Guide-for-Leaders.pdf
91.
https://ascopubs.org/doi/10.1200/EDBK_389516
92. https://pmc.ncbi.nlm.nih.gov/articles/PMC11698107/
93. http://ejpch.org/ejpch/article/view/693
94. https://www.alivewithideas.com/blog/change-and-chaos-the-fuel-of-creativity-and-a-spark-of-innovation/
95. https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.26.3.716?view=long&pmid=17485749
96. https://healthcaretransformers.com/healthcare-business/resource-management/nicholas-webb-chaotic-innovation-in-healthcare/
97. https://journals.stfm.org/familymedicine/2021/september/stange-2020-0588/
98. https://www.sciencedirect.com/science/article/pii/S0890509620304519
99. https://bmjopen.bmj.com/content/11/5/e048201
100.
https://scholarlycommons.hcahealthcare.com/cgi/viewcontent.cgi?article=1816&context=hcahealthcarejournal
101.
https://drug-card.io/blog/the-butterfly-effect-in-pharmacovigilance-small-data-big-impact/
102.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11225364/
103.
https://www.tcare.ai/resources/cancer/how-to-provide-emotional-support-to-a-loved-one-battling-cancer
104.
https://scholarworks.seattleu.edu/cgi/viewcontent.cgi?article=1073&context=dnp-projects
105.
https://www.sciencedirect.com/science/article/pii/S2059702924012651