ESMO Oncology Updates: What’s New in Cancer Treatment This Week
The latest European Society for Medical
Oncology (ESMO) research is reshaping how we treat cancer across multiple tumor
types. Here’s a breakdown of the most exciting advances—explained in practical
terms for your clinic and patients.
Head and Neck Cancer: Adding More
Immunotherapy = Better Outcomes
For years, we’ve relied on single
checkpoint inhibitors for head and neck cancer. That’s changing fast.
The Big
News: Combo Immunotherapy Works
Multiple trials presented at ESMO 2025
show that combining immunotherapy drugs—either before or after surgery—gives
better results than surgery alone.[1][2]
The KEYNOTE-689 trial tested pembrolizumab given before and after
surgery in patients with advanced, resectable head and neck cancer. Results? A
3-year event-free survival rate of 60% with combo therapy versus 46% with
surgery alone. Even better: about 9% of patients had complete pathologic
response (tumor nearly gone at surgery), compared to 0% in the surgery-only
group.[1]
What does
this mean for you?
·
Consider
perioperative immunotherapy for patients with locally advanced disease
·
Quality-of-life
data shows faster recovery with this approach
·
This is
now becoming standard of care in many centers
The
Emerging Trend: Why Stop at One Drug?
New research shows dual checkpoint
inhibitors—combining different immune targets—may overcome resistance. Trials
testing:
·
Retifanlimab + LAG-3 and TIM-3 blocking: Higher response rates than
single-agent PD-1 inhibitors
·
Tiragolumab (TIGIT blocker) +
atezolizumab: Early
promise in recurrent/metastatic disease
·
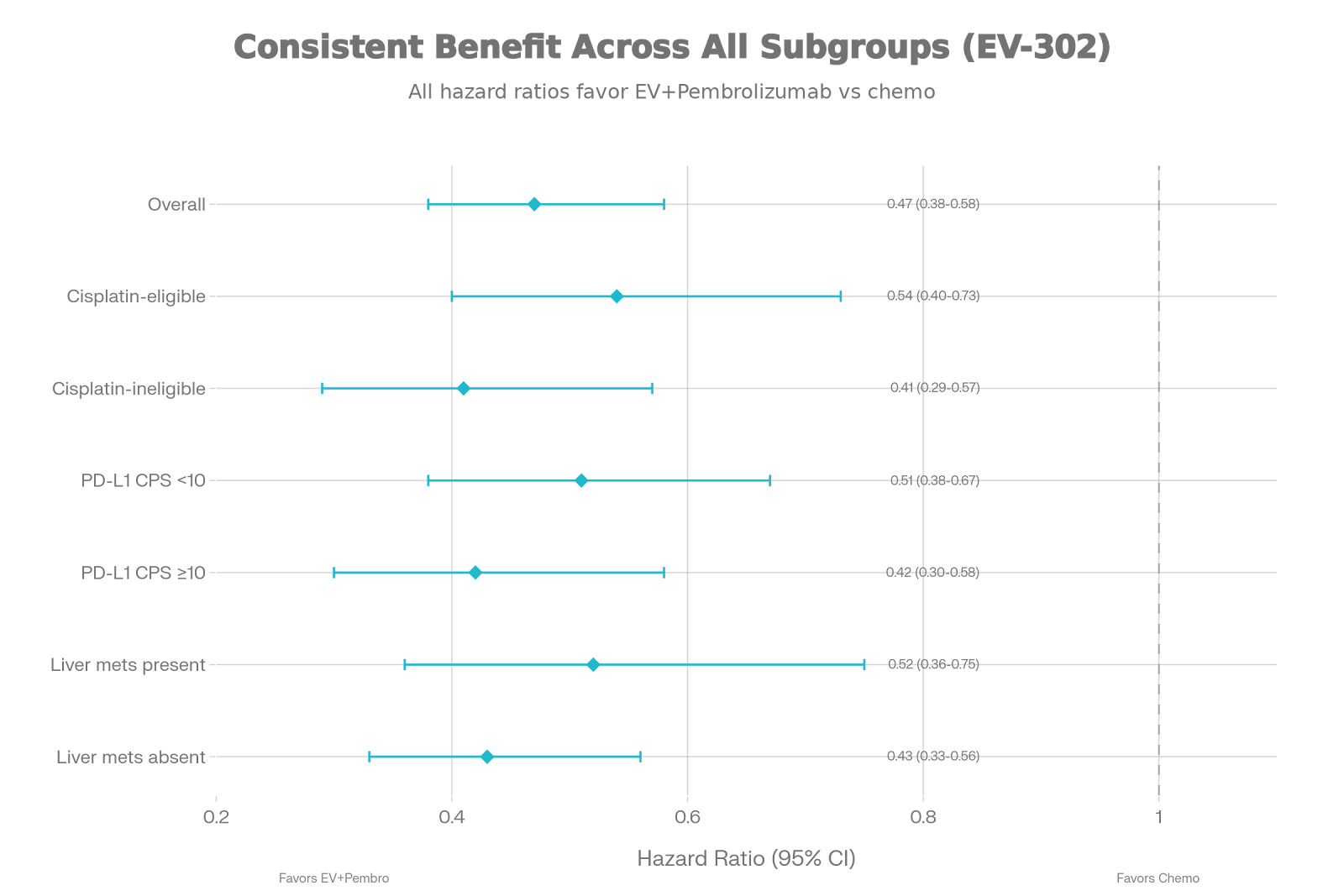
Enfortumab vedotin (a targeted drug) +
pembrolizumab: Novel
antibody-drug combination showing activity in first-line metastatic disease[1]
Bottom
line: Single-agent checkpoint
inhibition is becoming outdated. Combinations are the future.
Gastric Cancer: The Claudin 18.2
Revolution
This is perhaps the most transformative
area in upper GI oncology right now.
What is
claudin 18.2?
It’s a protein on the surface of gastric cancer cells that’s almost never
present in healthy stomach cells—making it a perfect target.
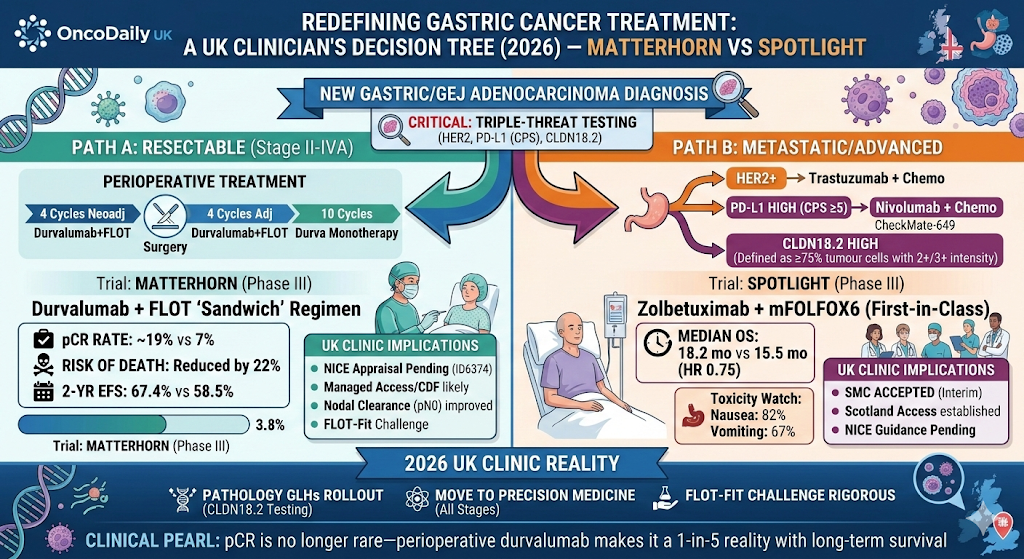
The
MATTERHORN Trial: Durvalumab-FLOT Now Standard
Adding durvalumab (a PD-L1 inhibitor)
to standard FLOT chemotherapy before surgery improved overall survival by 7% at
3 years (HR 0.78). The FDA has already approved this combination, making it the
new treatment standard for resectable gastric and gastroesophageal cancer.[3]
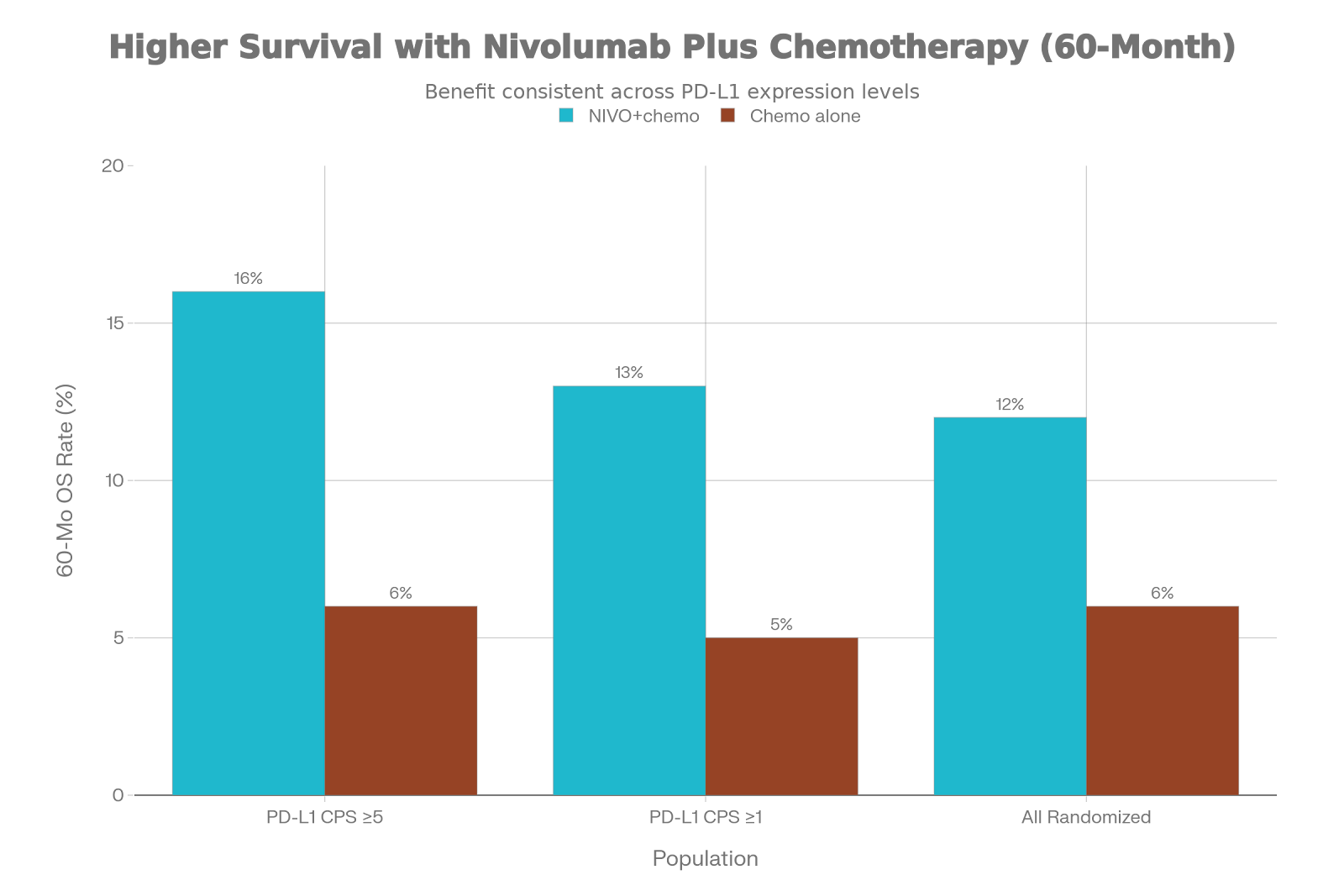
Key Point: This benefit worked regardless of
PD-L1 tumor status—unusual for immunotherapy and important for patient
selection.
The
Game-Changer: New Claudin 18.2 Drugs
Presented at ESMO Asia Congress
December 2025, JS107 (a claudin
18.2-targeting antibody) combined with immunotherapy and chemotherapy achieved
an 87% response rate in patients with high claudin 18.2 expression. Patients
are living longer, with median progression-free survival of 11 months.[4]
ASP2138 (another claudin 18.2 drug) is moving
into phase III trials. Early data suggest it works as monotherapy and in
combinations. Phase III enrollment expected mid-2026.[5]
What this
means:
·
Testing
tumors for claudin 18.2 should become routine
·
Patients
with high expression will benefit from new targeted combinations
·
This
could replace traditional chemotherapy-only approaches
Esophageal Cancer: Immunotherapy is
Standard, But Questions Remain
For metastatic esophageal squamous cell
carcinoma with high PD-L1 expression, platinum chemotherapy + anti-PD-1 therapy
is now standard first-line treatment.[6]
The unmet
need? We still don’t have a clear
optimal strategy after chemoradiotherapy fails. ESMO 2025 presentations
explored this question, with new trial designs being refined for 2026
enrollment.
Liver Cancer: Triple Combinations
Outperform Dual Therapy
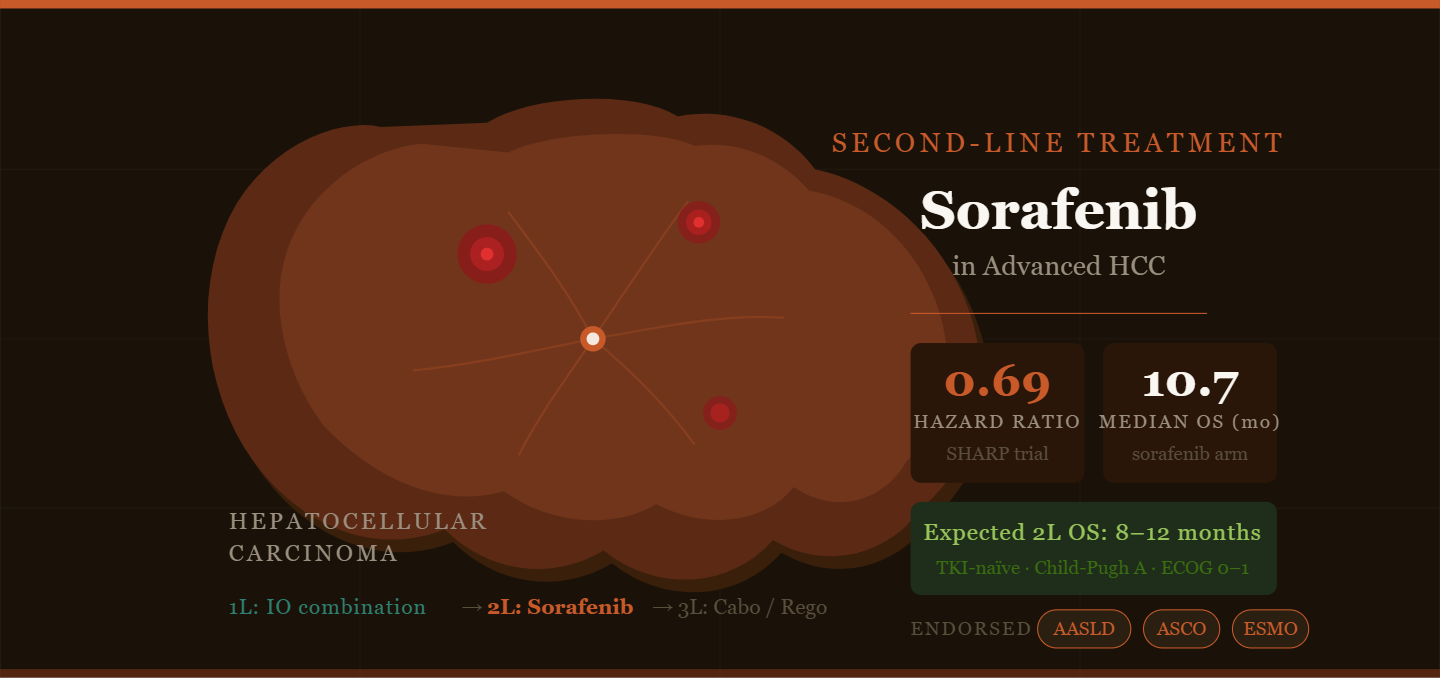
For
Advanced HCC
The gold standard has been atezolizumab
+ bevacizumab. Now, adding a third drug is showing promise.
The SKYSCRAPER-14 (IMbrave152) trial added tiragolumab (TIGIT
inhibitor) to atezolizumab-bevacizumab, improving response rates from 11% to
43%. This isn’t just about more responses—patients are staying on therapy
longer with durable control.[7]
ABC-HCC
Trial: Immunotherapy Beats Locoregional Therapy?
Here’s a stunning finding: In
intermediate-stage HCC, atezolizumab-bevacizumab delayed disease progression
longer than the traditional approach of TACE (a locoregional procedure). This
challenges decades of practice standards and suggests systemic immunotherapy
could replace TACE in selected patients.[7]
For Bile
Duct Cancer
The combination of toripalimab + lenvatinib + GEMOX chemotherapy achieved an 80%
response rate in intrahepatic cholangiocarcinoma with median overall survival
of 22.5 months. Some patients even became surgical candidates after this
intensive therapy—rare in biliary cancers.[7]
For advanced biliary tract cancer after
chemotherapy fails, durvalumab +
tremelimumab (dual checkpoint blockade) offers a late-line option, though
with modest 10% response rates and 8-month median survival.[7]
Bladder Cancer: Surgery is No Longer
Enough
KEYNOTE-905:
Antibody-Drug Combos Change the Game
For muscle-invasive bladder cancer, enfortumab vedotin + pembrolizumab
given before surgery dramatically improved outcomes.[8]
The
Results:
·
57% of
patients had complete pathologic response (cancer gone at surgery)
·
Compare
that to 9% with surgery alone—a 6-fold difference
·
Event-free
survival significantly improved
·
Surgery
was still safe and feasible
This represents a major shift toward
giving targeted drug + immunotherapy upfront to “shrink” tumors
before surgery.
POTOMAC:
BCG Plus Immunotherapy for Early Disease
For high-risk non-muscle-invasive
bladder cancer (early stages), adding durvalumab to BCG immunotherapy reduced
recurrence risk by 32%. This is the first successful blend of checkpoint
inhibition with BCG—the traditional treatment since the 1970s.[8]
What This
Means for Practice:
·
Early
MIBC: Consider perioperative immunotherapy
·
NMIBC:
BCG + durvalumab is now standard
·
Precision
approach: ctDNA-guided adjuvant therapy shows promise (IMvigor011 trial)—treat
only those who need it
Kidney Cancer: Triple Therapy and
Adjuvant Options Expand
First-Line
Triple Combinations
The KEYMAKER-U03 trial tested belzutifan (HIF-2α inhibitor) +
pembrolizumab + lenvatinib in untreated advanced kidney cancer. Results:
31.8-month median progression-free survival, outperforming dual therapy (20.8
months).[8]
Translation: More intensive upfront therapy delays
progression, but comes with more toxicity (70% grade 3+). Careful patient
selection is needed.
Adjuvant
(Post-Surgery) Therapy
The RAMPART trial showed that adjuvant durvalumab + tremelimumab (dual
checkpoint blockade) after surgery improves disease-free survival in high-risk
kidney cancer versus observation alone.[8]
For
Prostate Cancer
The EMBARK trial demonstrated that enzalutamide + leuprolide for
high-risk, biochemically recurrent prostate cancer achieved 79% 8-year overall
survival versus 70% with hormone therapy alone—a meaningful survival benefit
maintained over nearly a decade.[8]
The ICI Resistance Problem (And
Solutions)
What happens when patients stop
responding to checkpoint inhibitors? ESMO 2025 presented exciting new
strategies.
GDF-15
Neutralization: Visugromab + Nivolumab
The GDFATHER-01 trial identified GDF-15—a “don’t eat me”
signal cancer cells produce—as a resistance mechanism to PD-1 inhibitors.
Adding visugromab (anti-GDF-15) to nivolumab in ICI-refractory patients
achieved:
·
61.5%
complete/near-complete response rates
·
Median
response duration of 32+ months
·
Responses
deeper than patients’ initial immunotherapy[9]
What this
means: We may be able to
“rescue” patients who’ve already progressed on checkpoint
inhibitors—a significant advance in a desperate situation.
mRNA
Vaccine Approach: mRNA-4359 + Pembrolizumab
An mRNA vaccine encoding tumor antigens
(PD-L1 and IDO1) combined with pembrolizumab showed 67% response rates in
ICI-resistant melanoma. Remarkably safe with minimal toxicity despite prior
heavy immunotherapy exposure.[9]
VISTA
Inhibitors: A Different Checkpoint
Solnerstotug (anti-VISTA) combined with cemiplimab
in PD-L1-refractory patients achieved 14% response rate—proof that targeting
different immune pathways can overcome resistance.[9]
Bispecific
Antibodies: Dual Pathway Blocking
INCA33890 simultaneously blocks PD-1
(immunosuppression) and TGFβR2 (tumor-suppressive microenvironment). This dual
targeting addresses both immune cell exhaustion and immune exclusion—a
sophisticated approach to truly “cold” tumors.[10]
Skin Cancer: The Immunotherapy Era
Arrives
Squamous Cell Carcinoma: Adjuvant
Therapy Now Standard
The C-POST trial is practice-changing. For high-risk cutaneous squamous
cell carcinoma (cSCC) after surgery, adjuvant
cemiplimab significantly reduced recurrence and death:
The
Numbers:
·
2-year
disease-free survival: 87% with cemiplimab vs. 64% with placebo
·
68%
reduction in recurrence/death risk
·
Benefit
consistent across all patient subgroups, even PD-L1-negative tumors
·
Well-tolerated
with no surprise toxicities[11]
FDA
Approval: October
2025—cemiplimab is now the first-line adjuvant standard for high-risk cSCC,
replacing observation and older approaches.
For Your
Practice:
·
Risk
stratify all cSCC patients using established criteria (size, depth, grade,
margins, lymph node involvement)
·
High-risk
patients should receive 12 weeks of cemiplimab induction, then 6-week
maintenance dosing
·
Quality
of life improved compared to observation
Basal Cell Carcinoma: Options Beyond
Hedgehog Inhibitors
For advanced metastatic BCC, cemiplimab
offers durable disease control in patients intolerant to or progressing on
hedgehog pathway inhibitors (vismodegib, sonidegib).[12]
Merkel Cell Carcinoma: First Adjuvant
Immunotherapy Trial Shows Benefit
STAMP
Trial: Pembrolizumab After Surgery
This is the first phase III trial of
adjuvant immunotherapy in Merkel cell carcinoma (a rare, aggressive
neuroendocrine skin cancer). Results:[13]
·
Pembrolizumab
significantly reduced distant metastasis risk (HR 0.58; P=0.032)
·
Particularly
helpful for patients NOT receiving radiation therapy
·
Safety
acceptable (31% grade 3+ adverse events)
·
Overall
survival data pending
For
Metastatic Merkel Cell Carcinoma:
Long-term data from JAVELIN Merkel 200 shows avelumab
(first-line standard) achieves 4-year overall survival of 38%—remarkable
improvement over chemotherapy’s 10-14 months.[14]
Bonus Finding: Thymic Health Predicts
Immunotherapy Response
Research presented at ESMO 2025
discovered that thymic (immune organ) health correlates with better response to
checkpoint inhibitors. This opens future possibilities for optimizing
immunotherapy timing or potentially supporting thymic function in patients.[15]
Key Takeaways for Your Practice
1.
Perioperative Immunotherapy is Here
·
Moving
from salvage to curative-intent settings
·
HNSCC,
gastric cancer, and bladder cancer all benefit
·
Works
best with high-risk disease
2.
Combination Immunotherapy > Single Agent
·
Dual
checkpoint blockade (PD-1 + LAG-3, TIGIT, TIM-3, VISTA)
·
Combined
with targeted drugs (ADCs, kinase inhibitors)
·
Works for
both first-line and resistant disease
3.
Claudin 18.2 Testing is Essential
·
New
target in gastric cancer with excellent response rates
·
Test all
gastric/GEJ tumors
·
Multiple
drug options emerging
4.
Adjuvant Immunotherapy is Standard for Skin Cancers
·
High-risk
cSCC: cemiplimab is now approved
·
Merkel
cell: adjuvant pembrolizumab showing benefit
5.
Overcoming Resistance is Possible
·
GDF-15
neutralization, mRNA vaccines, new checkpoints
·
New
bispecific antibodies targeting dual pathways
·
Heavily
pretreated patients aren’t without options
6.
Precision Biomarkers Matter More Than Ever
·
PD-L1
status less predictive for some indications
·
ctDNA-guided
adjuvant therapy shows promise
·
Tumor-specific
targets (claudin 18.2) increasingly important
Phase III trials are underway for:
·
ASP2138
(claudin 18.2) in gastric cancer
·
Multiple
VISTA and TGFβR2 combinations
·
Expanded
indications for ADCs across tumor types
The oncology landscape is evolving
rapidly toward earlier, more intensive, biomarker-informed treatment—with
better outcomes and manageable side effects.
Bottom
line: 2025–2026 marks a transition
from broad checkpoint inhibition to precision medicine with rational
combinations designed for specific tumor vulnerabilities. Staying current with
these advances is essential for delivering cutting-edge care.
Key
References:
OncoDaily. “Top immunotherapy
trials ESMO 2025 head and neck.”[1]
Cancer Therapy Advisor. “ESMO 2025
Head and Neck Cancer News.”[2]
Cromospharma. “ESMO 2025 Insights:
What Will Really Change Oncology in 2026.”[3]
YouTube. “Upper GI cancer
highlights from ESMO 2025.”[6]
ESMO Daily Reporter. “New Claudin
18.2 approach shows promise in gastric cancer.”[4]
PMC NIH. “CLDN18.2-Targeted
Therapy in Gastrointestinal Cancers.”[5]
ESMO Daily Reporter. “Mixed
outcomes with novel targeted therapies for HER2+ upper GI.”[16]
EMJ Reviews. “ESMO 2025 Abstract
Highlights.”[17]
Digestive Cancers EU. “Progress in
Liver and Bile Duct Cancer: New Insights from ESMO 2025.”[7]
Urology Times. “ESMO 2025 recap:
Top trials in genitourinary oncology.”[8]
ESMO Daily Reporter. “Novel
strategies show promise in overcoming resistance to immune checkpoint
inhibitors.”[9]
OncoDaily. “Everything You Need to
Know About Immunotherapy at ESMO 2025.”[10]
OncoDaily. “Cemiplimab Gains FDA
Approval for Adjuvant High-Risk CSCC.”[11]
PubMed. “Cemiplimab in the
treatment of metastatic basal cell carcinoma.”[12]
JNCCN. “ESMO 2025: First Phase III
Data on Adjuvant Immunotherapy in Merkel Cell Carcinoma.”[13]
Merkelcell.org. “First-line avelumab treatment
in patients with metastatic Merkel cell carcinoma: 4-year results.”[14]
ESMO. “Study Shows Thymic Health
is Linked to Cancer Patients’ Response to Immunotherapy.”[15]
1.
https://www.esmo.org/meeting-calendar/esmo-congress-2026
2.
https://oncodaily.com/oncolibrary/immune-oncology/esmo-2025-head-and-neck
3.
https://www.clinicbarcelona.org/en/news/new-esmo-clinical-guidelines-for-the-diagnosis-and-treatment-of-hepatocellular-carcinoma
4.
https://dailyreporter.esmo.org/esmo-congress-2025/opinions/head-and-neck-cancers-should-research-continue-to-invest-in-immunotherapy
5.
https://oncodaily.com/oncolibrary/liver-and-pancreatic-cancer-trials-esmo25
6.
https://www.esmo.org/meeting-calendar/esmo-targeted-anticancer-therapies-congress-2026
7.
https://digestivecancers.eu/progress-in-liver-and-bile-duct-cancer-new-insights-from-esmo-2025/
8.
https://www.esmo.org/about-esmo-meetings/esmo-congresses
9.
https://oncologypro.esmo.org/webinars/esmo-congress-highlights-webinar-thoracic-head-neck-and-melanoma-cancers-2025
10.
https://www.oncologypipeline.com/apexonco/esmo-2025-preview-astellass-third-claudin182-shot
11.
https://www.instagram.com/p/DP0y0dTjKoe/
12.
https://www.esmo.org/meeting-calendar/esmo-congress-2025/abstracts
13.
https://www.esmo.org/guidelines/esmo-clinical-practice-guideline-biliary-tract-cancer
14.
https://www.esmo.org/meeting-calendar/esmo-gynaecological-cancers-congress-2026
15.
https://www.eortc.org/blog/2025/10/21/eortc-trials-presented-at-esmo-2025/
16.
https://www.esmo.org/meeting-calendar/esmo-sarcoma-and-rare-cancers-congress-2026/registration
17.
https://www.cancertherapyadvisor.com/features/esmo-2025-head-and-neck-cancer-news-key-takeaways/