Weekly Oncology Literature Round-Up 8–15 February 2026 | Key Journals Scan
Weekly
Oncology Literature Round-Up
8–15 February 2026 | Key Journals Scan
🔵 JAMA
Oncology
1. Induction vs
Adjuvant Chemoradiotherapy in High-Risk N2–N3 Nasopharyngeal Carcinoma (Phase 3
RCT)
Guo S, Li X, Liu L et al. JAMA Oncol. 2025;11(8):864–873[1]
•
Design: Open-label, phase 3 trial at Sun Yat-sen University (n = 324); EBV
DNA ≥1500 copies/mL; T1-4N2-3M0.
•
Arms: Paclitaxel–cisplatin–5FU induction → concurrent CRT vs
concurrent CRT → cisplatin–5FU adjuvant (3 cycles each).
•
Key result: No significant PFS difference — 3-year PFS 73.5%
(induction-concurrent) vs 70.4% (concurrent-adjuvant); HR 0.86 (95% CI
0.58–1.27; p = 0.45).
•
Toxicity: Comparable grade ≥3 leukopenia (33%) and mucositis (29%)
in both arms. Two treatment-related deaths in the induction group; none in the
adjuvant group.
•
Editorial comment (notable): Induction chemotherapy was associated with poorer local control,
while adjuvant PF was poorly tolerated leading to compromised distant control.
Adjuvant gemcitabine-cisplatin may be superior to adjuvant PF and potentially
equivalent to induction GP for distant control and OS. The editorial suggests a
future trial of upfront concurrent CRT + single-agent adjuvant
gemcitabine/capecitabine ± anti-EGFR for selected patients.
🩺 Bottom line for practice: If
you’re deciding between induction and adjuvant chemotherapy for high-risk NPC,
this trial suggests either sequence is reasonable — discuss with the
patient. Consider gemcitabine-based adjuvant regimens over PF if choosing the
adjuvant route.
2. Quality of
Life and Survival in First-Line Systemic Therapy for Advanced HCC (Network
Meta-Analysis)
Celsa C, Di Maria G, Lombardi P et al. JAMA Oncol. Published online
August 14, 2025[2]
•
Data: 9 phase 3 RCTs, 6425 patients; Bayesian NMA using sorafenib as
comparator.
•
Assessed: Time to deterioration across 7 HRQoL domains (EORTC QLQ-C30 and
HCC18) integrated with OS.
•
Key findings:
–
Atezolizumab + bevacizumab ranked highest for delaying deterioration in global health status
(SUCRA 85%), abdominal swelling (95%), jaundice (89%), and pain (86%).
–
Tislelizumab ranked best for physical functioning (96%) and fatigue.
–
When integrating QoL with OS,
atezo-bev outperformed all other treatments across all domains.
🩺 Bottom line for practice: This
provides the strongest composite evidence yet that atezolizumab +
bevacizumab remains the optimal first-line choice for advanced HCC when
considering both survival and quality of life — a valuable talking point for
MDT discussions and patient counselling.
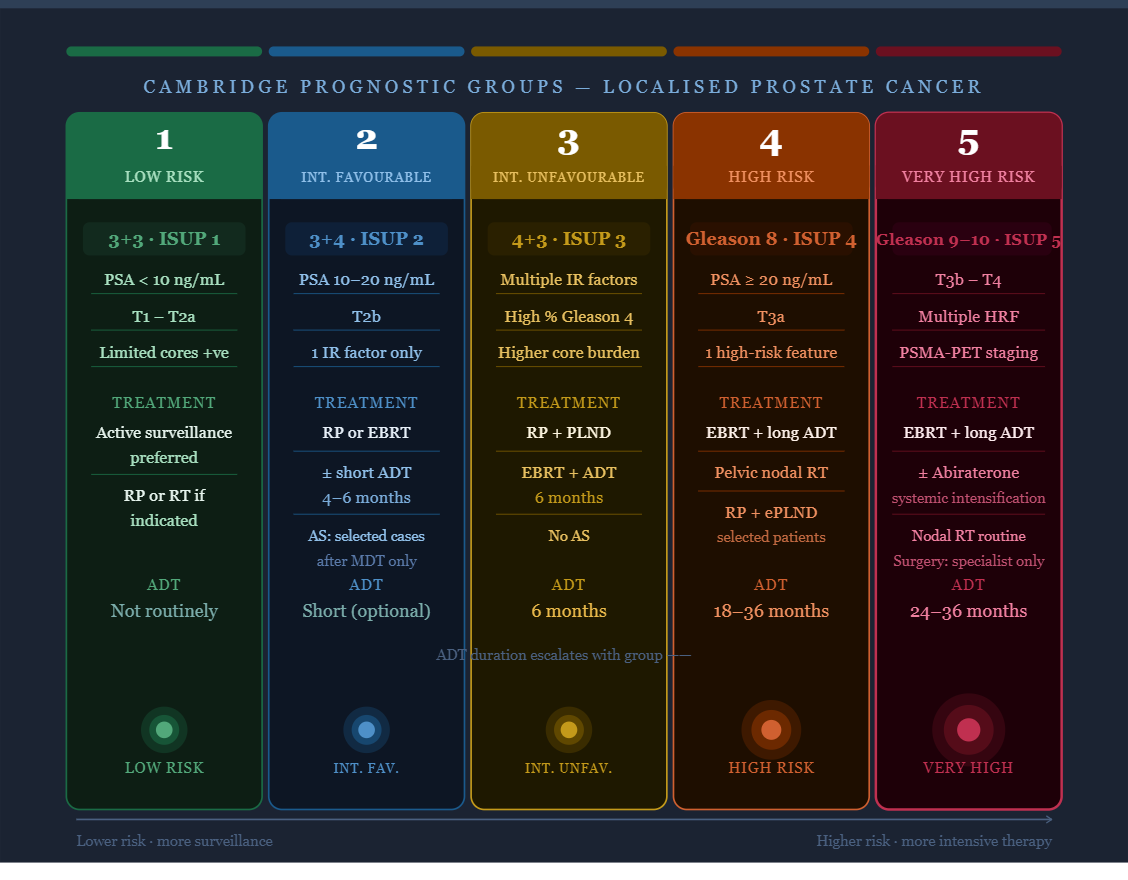
3. Prostate
Cancer Screening — MRI-Targeted Screening Viewpoint
JAMA Oncology (current issue)[3]
A
Viewpoint article discusses the need to optimise prostate cancer screening
strategies beyond PSA alone, advocating for more widespread use of MRI-targeted
screening to reduce unnecessary biopsies and overdiagnosis of clinically
insignificant disease. This aligns with growing UK evidence (e.g., ReIMAGINE,
GÖTEBORG-2 trial data) supporting MRI as a triage tool.
🩺 Bottom line: Reinforces the
evolving paradigm that PSA alone is insufficient; MRI-first pathways (already
being adopted in some NHS trusts) are gaining international momentum.
4. Mupirocin for
Radiation-Induced Oral Mucositis (RCT) — Head & Neck Relevant
JAMA Oncology (online first)[4]
A
randomised clinical trial evaluating bacterial decolonisation with mupirocin
nasal ointment to alleviate severe acute radiation oral mucositis during
head and neck radiotherapy. Full details behind paywall, but this is a notable
supportive care trial — mucositis remains a major dose-limiting toxicity and
quality-of-life burden during radical (chemo)radiotherapy for H&N cancers.
🔵 Nature
Reviews Clinical Oncology
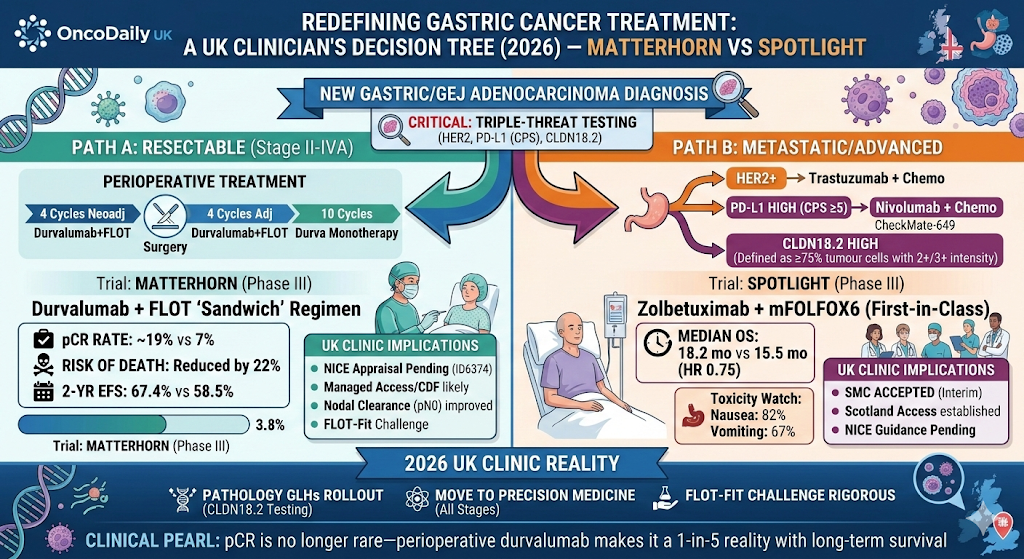
5. Anbenitamab:
A New Second-Line Option in Gastric/GEJ Adenocarcinoma
Nat Rev Clin Oncol (published 28 Jan 2026)
This
brief communication highlights anbenitamab, a bispecific antibody
targeting HER2 and HER3, as a new second-line treatment option for
gastric/gastroesophageal junction (G/GEJ) adenocarcinoma. This follows the
broader trend of HER2-directed therapies expanding in upper GI cancers beyond
trastuzumab/T-DXd.[5]
🩺 Bottom line: Another signal
that bispecific antibodies are reshaping the upper GI treatment landscape.
Watch this space for integration into treatment algorithms alongside
trastuzumab deruxtecan.
6. Advances in
the Management of Localised Bladder Cancers
Nat Rev Clin Oncol (published Jan 2026; correction published 11 Feb
2026)
A
comprehensive review by Marie-Pier St-Laurent, Jussi Nikkola, Peter C. Black
covering the evolving management of localised (non-muscle-invasive and
muscle-invasive) bladder cancer. The correction published on 11 Feb 2026
updates the original article.[6]
Key
themes likely covered:
•
Emerging role of pembrolizumab
and nadofaragene firadenovec for BCG-unresponsive NMIBC
•
Neoadjuvant immunotherapy +
chemotherapy combinations for MIBC
•
Bladder-sparing strategies
including trimodal therapy
7. ctDNA-Guided
Personalised Therapy for Muscle-Invasive Bladder Cancer
Nat Rev Clin Oncol (published Jan 2026)
A
review article by the same St-Laurent/Nikkola/Black group discussing circulating
tumour DNA as a guide for personalised therapy in MIBC — including its role
in MRD detection post-cystectomy, treatment escalation/de-escalation, and
monitoring during bladder-sparing approaches.
🩺 Bottom line (items 6 & 7):
Bladder cancer management is undergoing a paradigm shift. ctDNA-driven adjuvant
therapy decisions are moving closer to clinical practice (see also IMvigor011
and other ctDNA-directed trials).
🔵
Journal of Clinical Oncology (JCO)
8. Skin Cancer —
New Reports
The
JCO table of contents confirms at least two new Original Reports in Skin
Cancer published in the online-first section during this period. Full
titles were not extractable due to website rendering, but the articles appear
under the Skin Cancer category and are distinct from melanoma (relevant to your
interest in non-melanoma skin cancer).
9. Genitourinary
Cancer Reports
Multiple
articles are flagged under Genitourinary Cancer in the newest articles
section, including at least 3–4 original reports. These likely cover prostate
and/or bladder cancer topics.
10. CodeBreaK
300 Overall Survival Update — KRAS G12C CRC
Visible on the JCO homepage — Overall
survival analysis of the phase III CodeBreaK 300 study (sotorasib + panitumumab
vs investigator’s choice in chemorefractory KRAS G12C colorectal cancer). While
not in your specific tumour-site list, this is a practice-relevant update in GI
oncology.
🔵 Lancet
Oncology & Annals of Oncology
Both
journals’ websites were blocked by Cloudflare protections during this search.
Based on general availability:
•
Lancet Oncology typically publishes its monthly issue mid-month (the February 2026
issue would be expected around now), with online-first articles appearing
continuously.
•
Annals of Oncology similarly has rolling online publications.
I
was unable to confirm specific article titles from these journals for the 8–15
February window. I would recommend checking these directly:
•
🔗 Lancet
Oncology Online First
•
🔗 Annals
of Oncology In Press
Quick-Reference Summary
Table
|
# |
Journal |
Topic |
Key |
|
1 |
JAMA |
NPC: |
No PFS |
|
2 |
JAMA |
HCC: QoL |
Atezo-bev |
|
3 |
JAMA |
Prostate |
Push for |
|
4 |
JAMA |
H&N: |
RCT of |
|
5 |
Nat Rev |
Upper GI: |
New |
|
6 |
Nat Rev |
Bladder |
Comprehensive |
|
7 |
Nat Rev |
Bladder |
MRD-directed |
|
8–9 |
JCO |
Skin Ca |
New |