Weekly Journal Scan : Keep up to date
Latest Updates from Major Medical Journals
December
2025 Summary
This comprehensive review synthesizes
critical clinical trial data from the world’s leading oncology journals,
highlighting transformative immunotherapy strategies across seven major cancer
types. The evidence reveals a paradigm shift toward precision-guided combination therapies, neoadjuvant immunotherapy, and molecular
biomarker-driven patient selection.
Bottom
Line: Immunotherapy integration is now
standard across early and advanced stages, with emerging data supporting
intelligent combination approaches and de-escalation strategies.
🔴 NON-MELANOMA SKIN CANCER
(Cutaneous Squamous Cell Carcinoma)
Anti-PD-1/PD-L1 checkpoint inhibitors
have transformed the management of advanced cutaneous squamous cell carcinoma
(CSCC), moving this disease from a historically challenging field to one with
reproducible, durable responses.
|
Trial |
Setting |
Key |
Clinical |
|
C-POST |
Adjuvant CSCC |
Improved disease-free survival; n=415 |
✅ Established adjuvant immunotherapy standard |
|
De-Squamate |
Neoadjuvant CSCC |
63% pCR + cCR; RT avoidance 48% |
✅ Enables surgical de-escalation |
|
Alliance |
Advanced CSCC |
Avelumab + cetuximab vs monotherapy |
✅ Exploring EGFR synergy |
|
Cosibelimab |
Advanced CSCC |
ORR 47.5%; mPFS 12.9 months |
✅ New PD-L1 inhibitor option |
Neoadjuvant Immunotherapy—Game Changer
Pooled
Analysis Results:
Anti-PD-1 neoadjuvant therapy across 17 cancer centers
·
Pathological complete response (pCR): 37–55%
·
Major pathological response (≤10%
viable tumor): 56%
·
Benefit: Significant de-escalation or avoidance of postoperative
radiotherapy
De-Squamate
Trial Highlights:
·
63% combined pCR + clinical complete
response
·
48% avoided postoperative RT
·
15% achieved complete RT avoidance
·
Functional outcomes: Improved cosmesis and quality of life
✓ Neoadjuvant immunotherapy is now standard for high-risk resectable CSCC
✓ Adjuvant cemiplimab proven for post-surgical disease
✓ Combination with EGFR inhibitors shows promise for advanced disease
🎤 HEAD & NECK SQUAMOUS CELL CARCINOMA
Dual-Checkpoint Inhibitors Enter
Clinical Practice
Recent trials are pivoting from
single-agent PD-1 inhibition to dual-mechanism
combinations targeting complementary immune pathways.
1. Dual Immune Checkpoint Inhibitors
A phase II randomized trial compares
three neoadjuvant approaches in locally
advanced resectable HNSCC:
|
Agent |
Mechanism |
Partner |
|
Ivonescimab |
PD-1/VEGF bispecific |
Cisplatin + nab-paclitaxel |
|
Cadonilimab |
PD-1/CTLA-4 bispecific |
Cisplatin + nab-paclitaxel |
|
Penpulimab |
PD-1 monotherapy |
Cisplatin + nab-paclitaxel (control) |
Rationale: Dual targets aim to overcome
compensatory immune checkpoint upregulation and enhance T-cell infiltration.
2. Neoadjuvant Cemiplimab (NeoPOWER
Trial)
Patients with high-risk/unresectable
cutaneous SCC of the head and neck:
·
Pathologic complete response → 92%
disease-free survival at 12 months
·
Supports surgical de-escalation and organ preservation
·
Functional outcomes: Reduced need for extensive surgical
reconstruction
3. Novel TLR-7 Agonist Approach
Neoadjuvant imiquimod in oral squamous
cell carcinoma:
·
60% achieved ≥50% tumor cell reduction
·
60% immune-related major pathologic
response
·
1-year RFS: 93%
·
Tolerability: Excellent
Why This
Matters:
Toll-like receptor activation activates dendritic cells through different
pathways than checkpoint inhibition, potentially addressing heterogeneous tumor
immunity.
✓ Dual-checkpoint combinations now
entering phase 2/3 trials
✓ Neoadjuvant approach enables surgical
de-escalation
✓ Consider TLR agonists in select oral cancers
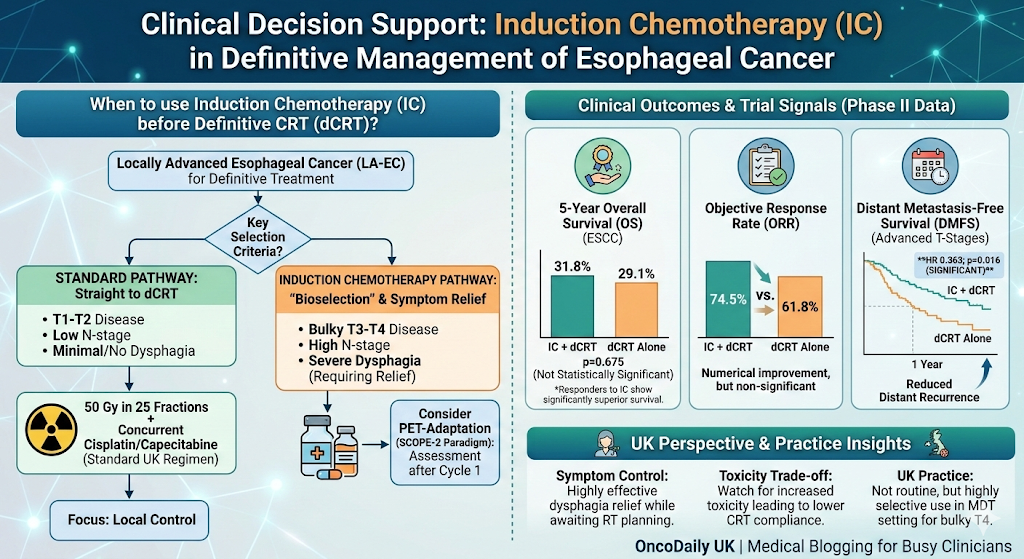
🫔 UPPER GASTROINTESTINAL CANCER
(Gastric & Esophageal)
Immunotherapy is Now Multi-Setting
Immunotherapy has expanded from
metastatic disease to neoadjuvant,
adjuvant, and combination settings, redefining the management of gastric
and esophageal cancers.
Durvalumab
+ DOS (Docetaxel/Oxaliplatin/S-1) in Locally Advanced Gastric Cancer
|
Metric |
Result |
|
Phase |
Phase II (n = TBD) |
|
Primary |
Met |
|
Pathologic |
Favorable pCR rates |
|
Next |
Phase III planned for Asian populations |
|
Implication |
Standard platform for locally advanced gastric cancer |
PARAMUNE
Trial (SWOG 2303)
Treatment: Nivolumab + Paclitaxel + Ramucirumab vs. Paclitaxel + Ramucirumab
For PD-L1
CPS ≥1 Advanced Gastric/Esophageal Adenocarcinoma:
|
Metric |
With |
Without |
|
Median |
6.4 months |
5.1 months |
|
Median |
13.8 months |
8.0 months |
|
Improvement |
+1.3 mo PFS, +5.8 mo OS |
— |
✅ Triple
combination adds meaningful survival benefit
FIRST-LINE PD-L1-POSITIVE ESOPHAGEAL
CANCER
KEYNOTE-181
& KEYNOTE-590:
·
Pembrolizumab vs. chemotherapy in PD-L1 CPS ≥1 esophageal SCC
·
Higher objective response rates with immunotherapy
·
Durable remissions in responsive patients
HER2-Positive
Gastric/GEJ Cancer (KEYNOTE-811):
·
Pembrolizumab + Trastuzumab +
Chemotherapy
·
Improved ORR vs. chemotherapy + trastuzumab alone
·
New standard for HER2+ metastatic
disease
Tislelizumab
in Esophageal SCC (2nd Line)
·
Comparative
efficacy data emerging
·
Potential
alternative for PD-1-naïve patients
·
Ongoing
head-to-head trials
🧬 EMERGING: GUT MICROBIOTA ENGINEERING
Antibiotic-Assisted
Fecal Microbiota Transplantation Before Immunotherapy
·
Hypothesis:
Restore immunogenic commensals before ICI
·
Mechanism:
Enhanced DC activation & CD8+ T-cell infiltration
·
Status: Early-phase investigation
✓ Neoadjuvant
durvalumab + chemotherapy is standard for locally advanced disease
✓ Nivolumab triplet provides
meaningful OS benefit in advanced PD-L1+ disease
✓ Pembrolizumab is first-line for
PD-L1+ esophageal SCC
✓ Gut microbiome optimization may enhance responses
Rapid Evolution Driven by Bispecific
Antibodies
Hepatocellular carcinoma and biliary
tract cancers are experiencing unprecedented progress with bispecific antibodies, PD-L1/CTLA-4
combinations, and precision
locoregional-systemic approaches.
HEPATOCELLULAR CARCINOMA (HCC)
DUAL-CHECKPOINT BISPECIFIC: KN046 +
Lenvatinib
|
Metric |
Result |
|
Mechanism |
PD-L1/CTLA-4 bispecific + VEGFR inhibitor |
|
Objective |
45.5% |
|
Median |
11.0 months |
|
Median |
16.4 months |
|
Biomarker |
ctDNA before cycle 3 predicts outcome |
Why
Noteworthy: First
dual-checkpoint bispecific in HCC showing efficacy comparable to or better than
standard atezolizumab/bevacizumab regimens, with potential for biomarker-driven
selection.
![]()
LOCOREGIONAL + SYSTEMIC: IMPACT Study
(Phase 3)
Patient
Population:
Unresectable HCC with stable disease on atezolizumab/bevacizumab
Intervention: Addition of Transarterial
Chemoembolization (TACE)
Rationale: Post-hoc analyses of IMbrave150
suggested benefit of adding locoregional therapy to systemic immunotherapy
✅ Precision
approach: Combines optimal timing of locoregional and systemic therapies
PERI-INTERVENTIONAL IMMUNOTHERAPY:
IMMULAB (Phase 2)
|
Setting |
Agent |
Locoregional |
Goal |
|
Early-stage |
Neoadjuvant Pembrolizumab |
RF ablation, microwave, brachytherapy |
Reduce recurrence; preserve liver |
Emerging
Options for Post-Immunotherapy Progression:
|
Regimen |
Agents |
Trial |
Setting |
|
Anlotinib |
VEGFR + PD-L1 inhibitor |
FAITH (Phase 2) |
Previously IO-treated |
|
Botensilimab |
Enhanced CTLA-4 + PD-1 |
Phase 1 |
PD on prior ICI |
Median
Follow-Up (Botensilimab): 11.4
months with encouraging durability and tolerability
ZANIDATAMAB—Game-Changer for HER2+ BTC
·
Dual HER2-targeted bispecific antibody
·
FDA accelerated approval achieved
·
Now entering Phase 3 (HERIZON-BTC-302)
Regimen: Zanidatamab + Cisplatin/Gemcitabine ±
PD-1/PD-L1 inhibitor
Population: HER2-positive advanced/metastatic BTC
(1st line)
Implication: First targeted therapy specifically
for HER2+ BTC; immunotherapy combinations being explored
✓ KN046
+ lenvatinib offers new option for advanced HCC
✓ Combine locoregional + systemic
therapy in appropriate patients
✓ Zanidatamab transforms HER2+
biliary tract cancer landscape
✓ Re-challenge strategies emerging
for post-IO progression
Multiple Immunotherapy Platforms in
Development
Prostate cancer has historically been
considered “immunologically cold,” but emerging data demonstrate
activity with dual immunomodulation,
vaccine-based approaches, and PARP/PD-L1 combinations.
1. HDAC Inhibition + Checkpoint
Blockade
Pembrolizumab
+ Vorinostat (Phase I/IB)
Patient
Population:
Metastatic prostate cancer, renal cancer, advanced urothelial carcinoma
Rationale:
·
Vorinostat
(HDAC inhibitor) reduces Treg and MDSC
populations
·
Creates
an immunopermissive microenvironment
·
Synergizes with PD-1 blockade
Status: Dose escalation and safety evaluation
ongoing
2. THERAPEUTIC VACCINE + CHECKPOINT
BLOCKADE
pTVG-HP +
Nivolumab (Phase 2)
|
Population |
Agent |
Target |
Status |
|
Biochemically |
DNA vaccine + PD-1i |
Prostatic acid phosphatase |
Active surveillance alternative |
Hypothesis: Vaccine priming + checkpoint blockade
reconstitutes T-cell immunity against tumor-associated antigens
![]()
3. DUAL-TARGETED STRATEGY: PARP + PD-L1
(mCRPC)
Durvalumab
+ Olaparib in Metastatic CRPC
Biomarker-Driven
Analysis:
·
Liquid biopsy: ctDNA dynamics, tumor fraction, immune
profiling
·
Identifies mechanisms of resistance
·
Informs patient selection for dual-targeted approach
Implication: Resistance mechanisms are increasingly
molecularly defined, enabling
personalized treatment planning
![]()
✓ HDAC
inhibitors open new immunomodulatory avenue
✓ Vaccine-based approaches may offer
alternative to ADT escalation
✓ Dual PARP/checkpoint inhibition
shows promise in select mCRPC
✓ Biomarker-guided selection is
emerging best practice
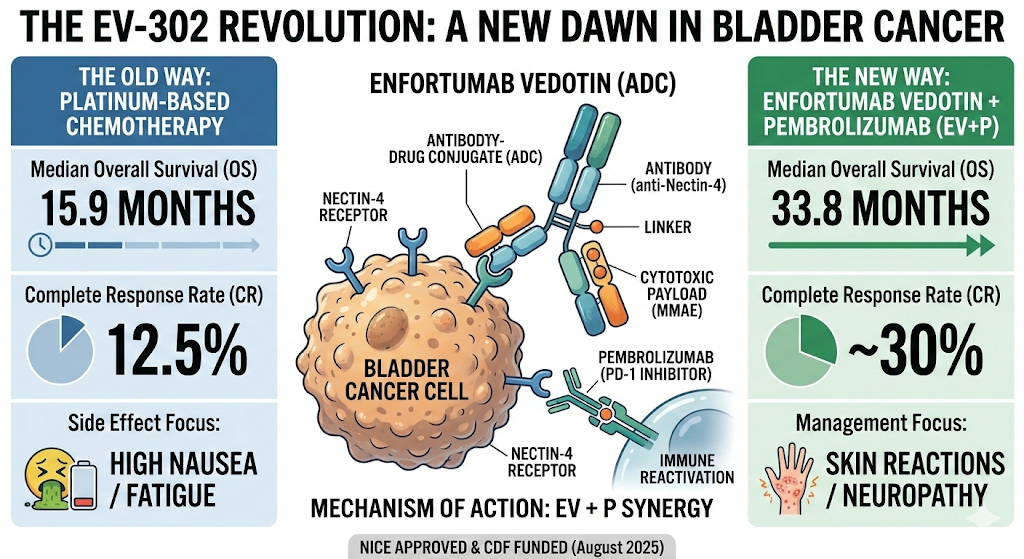
🟣 BLADDER CANCER (Muscle-Invasive)
Neoadjuvant Immunotherapy Redefines
Surgical Approach
Muscle-invasive bladder cancer (MIBC)
treatment is undergoing fundamental
restructuring with neoadjuvant chemo-immunotherapy, enabling organ preservation and risk-adapted approaches.
CHECKPOINT-BASED NEOADJUVANT THERAPY
AURA Trial: Avelumab-Based Regimens
|
Arm |
Chemotherapy |
Immunotherapy |
pCR |
3-Yr OS |
|
Arm 1 |
Dose-dense MVAC |
Avelumab |
58% |
87% |
|
Arm 2 |
Gemcitabine/cisplatin |
Avelumab |
53% |
67% |
Key
Finding: Chemotherapy intensity impacts long-term
survival
✅ Dose-dense MVAC appears superior to standard-dose GC in AURA
RETAIN-2: Risk-Adapted Precision
Medicine
Patient
Population:
Cisplatin-ineligible MIBC
Approach:
1. Induction: Nivolumab + MVAC chemotherapy
2. Assessment: Achieve clinical complete response?
o If YES +
DNA repair gene mutations (ATM, ERCC2, RB1): ✅ Active surveillance (bladder preservation)
o If NO or
wild-type:
Conventional radical cystectomy
Implication: Molecular
profiling guides treatment de-escalation
|
Trial |
Regimen |
Population |
Key |
|
NeoSTOP-IT |
Gem/Cis + cemiplimab ± fianlimab (anti-LAG-3) |
Cisplatin-eligible MIBC |
Exploring dual-checkpoint strategy |
|
FGFR + |
Futibatinib + durvalumab |
FGFR-overexpressing MIBC |
Targeting molecular subsets |
|
Sintilimab |
Sintilimab + Gem/Cis |
Cisplatin-eligible MIBC |
67.4% |
Sintilimab
Highlights:
·
Despite
high baseline T3-T4a disease burden
·
Predominantly
grade 1-2 irAEs
·
Remarkable
67.4% bladder preservation rate
ADVANCED/METASTATIC UROTHELIAL
CARCINOMA
AURORA
Trial: Atezolizumab in Urinary Tract SCC
·
Advanced squamous cell carcinoma of
bladder/urinary tract
·
High PD-L1 expression & immune
infiltration
·
Proof-of-concept: Atezolizumab monotherapy shows
activity in this rare subtype
✓ Dose-dense
MVAC + avelumab optimal for cisplatin-eligible patients
✓ Risk-adapted approach (molecular
profiling) guides de-escalation
✓ Dual anti-LAG-3/PD-1 may overcome
resistance
✓ 67% bladder preservation
achievable with chemo-immunotherapy
1. PRECISION ONCOLOGY INTEGRATION
✓ PD-L1
expression, TMB, MSI, DNA repair mutations inform patient selection
✓ Biomarker-driven de-escalation is
emerging standard
✓ ctDNA dynamics predict outcomes
and treatment response
2. DUAL-CHECKPOINT & BISPECIFIC
ANTIBODIES
✓ PD-1/CTLA-4,
PD-L1/CTLA-4 combinations show enhanced efficacy
✓ PD-L1/VEGF bispecifics (KN046)
redefine HCC landscape
✓ Requires careful toxicity monitoring
✓ Surgery
de-escalation now achievable across multiple cancer types
✓ Pathologic response emerges as surrogate for long-term survival
✓ Organ preservation drives improved
functional outcomes
✓ Circulating
tumor DNA predicts prognosis and response
✓ Spatial transcriptomics reveals
tumor core/edge dynamics
✓ Gut microbiota composition
influences immunotherapy efficacy
5. IMMUNOTHERAPY TOXICITY MANAGEMENT
✓ Immune-related
adverse events (irAEs) now systematically monitored
✓ TIL (tumor-infiltrating lymphocyte)
therapy emerging for select patients
✓ Systemic toxicity protocols
becoming standard of care
6. LOCOREGIONAL-SYSTEMIC INTEGRATION
✓ TACE
+ atezolizumab in HCC (IMPACT trial)
✓ Percutaneous ablation + pembrolizumab
in early-stage HCC (IMMULAB)
✓ Precision timing of locoregional
and systemic therapy is critical
|
Cancer |
Neoadjuvant |
Advanced |
Key |
|
Cutaneous |
PD-1 inhibitor ✓ |
Multiple agents available |
Dual-target combos |
|
Head |
Dual-checkpoint ✓ |
Combination strategies |
TLR-7 agonists |
|
Gastric/Esophageal |
Durvalumab + chemo ✓ |
Nivolumab triplet |
Microbiota engineering |
|
HCC |
Pembrolizumab + ablation |
KN046 + lenvatinib |
Bispecific antibodies |
|
BTC |
Not standard |
Zanidatamab (HER2+) |
Precision HER2 targeting |
|
Prostate |
Investigational |
PARP/PD-L1, vaccines |
Dual immunomodulation |
|
MIBC |
Chemo-IO ✓ |
Active surveillance |
Risk-adapted protocols |
1. Integrating
immunotherapy is now standard of care across these cancers
2. Molecular
profiling should guide therapy selection (PD-L1, TMB, DNA repair status, FGFR, HER2)
3. Neoadjuvant
immunotherapy enables surgical de-escalation—prioritize in appropriate patients
4. Dual-checkpoint
combinations show
promise but require toxicity vigilance
5. Biomarker-driven
de-escalation (e.g.,
RETAIN-2, risk-adapted approaches) preserves quality of life
6. Stay
informed on emerging trials—the
landscape evolves rapidly
This analysis synthesizes data from:
·
Journal of Clinical Oncology (JCO)
·
Annals of Oncology
·
The Lancet Oncology
·
JAMA Oncology
·
Nature Reviews Clinical Oncology
·
Nature Communications
·
Frontiers in Oncology & Immunology
·
American Society of Clinical Oncology
(ASCO) Meeting Archives
Published: December 2025
Subscribe to stay updated on the latest
immunotherapy breakthroughs across oncology.